
Cervical Disc Herniation
A cervical disc herniation happens when a disc in the neck bulges or ruptures and irritates nearby nerves. This can cause neck pain, radiating arm pain, numbness, tingling, or weakness.
Common Symptoms
- Neck pain or stiffness
- Pain traveling into the shoulder or arm
- Numbness or tingling in the hand or fingers
- Weakness in the arm or grip
Common Causes
- Age-related disc degeneration
- Poor posture and repetitive strain
- Injury (sports, falls, or car accidents)
- Heavy lifting or sudden twisting
What Is a Cervical Disc Herniation?
The cervical spine is the upper portion of the spine in the neck. Discs sit between vertebrae and act as shock absorbers. A herniation occurs when the disc’s inner material pushes through the outer layer and can irritate or compress a nerve root and sometimes the spinal cord.
Nerve irritation can cause neck pain that radiates into the shoulder, arm, or hand and may produce numbness, tingling, or weakness depending on the affected nerve level.
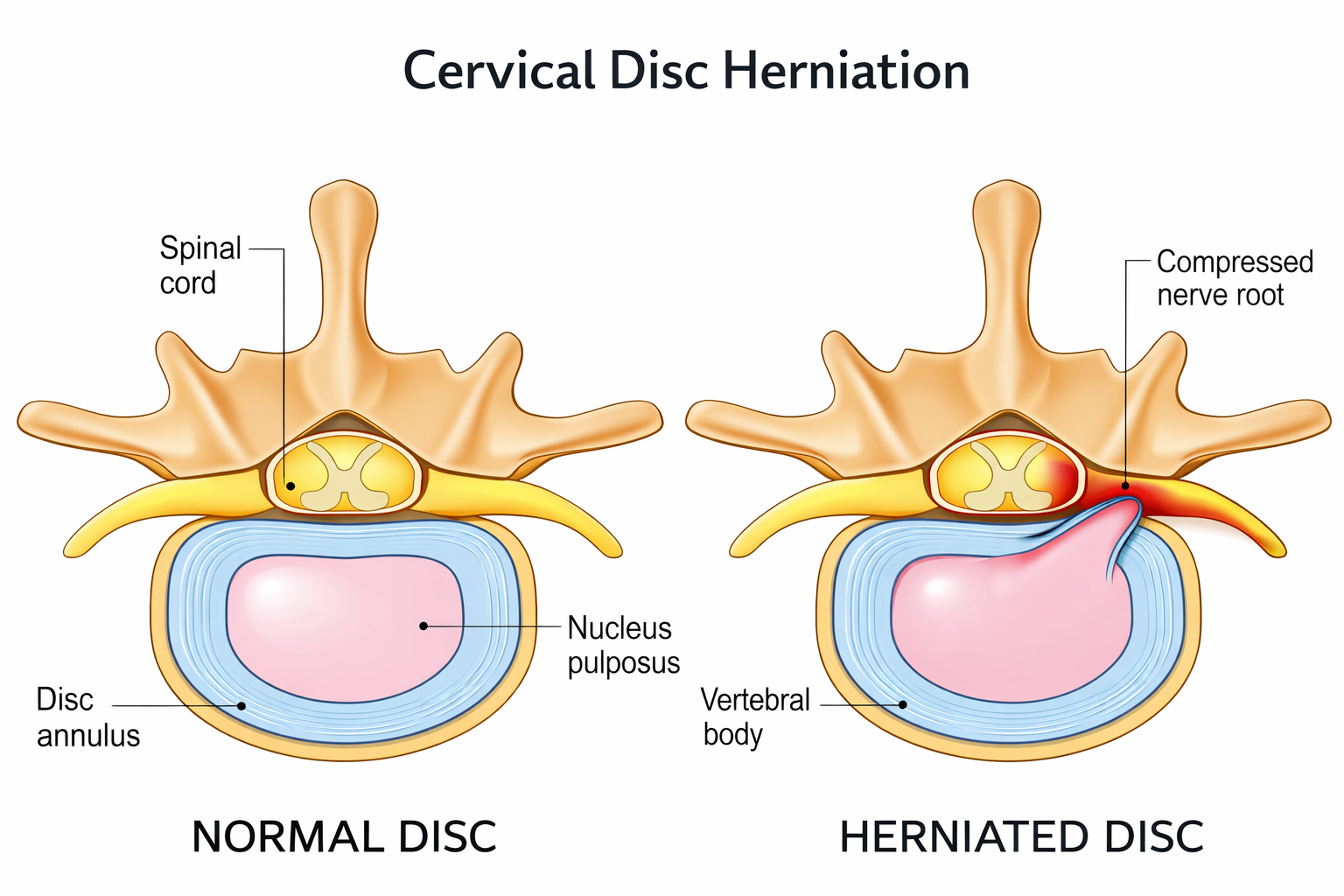
Illustration showing cervical disc herniation causing nerve compression.
Why It Hurts
When a nerve root is irritated, pain may travel down the arm (cervical radiculopathy). You may also notice numbness, tingling, or weakness depending on which nerve is affected.
Cervical RadiculopathyWhen It Needs Prompt Evaluation
Balance changes, hand clumsiness, coordination issues, or worsening weakness may suggest spinal cord involvement and should be evaluated promptly.
Diagnosis
Diagnosis starts with a focused physical exam and a review of your symptoms. Imaging helps confirm the level and severity of the herniation and whether a nerve root or the spinal cord is affected.
Clinical Exam
- Range of motion and pain pattern
- Strength, sensation, and reflex testing
- Nerve irritation tests (as appropriate)
Imaging
- MRI (best for discs and nerves)
- X-rays (alignment and degeneration)
- CT or CT myelogram (selected cases)
Additional Tests
- EMG/NCS (if needed for nerve function)
- Diagnostic injections (selected cases)
Treatment
Treatment usually starts with conservative care aimed at reducing inflammation and restoring function. If symptoms persist, or if weakness progresses, minimally invasive or surgical options may be recommended.
Non-Surgical Options
- Physical therapy (posture, strengthening, mobility)
- Activity modification and ergonomic changes
- Anti-inflammatory medications (NSAIDs) when appropriate
- Short-term oral steroids (selected cases)
- Muscle relaxants (for spasm-related pain)
- Cervical traction (when appropriate)
- Epidural steroid injections
- Selective nerve root blocks (targeted)
- Heat/ice and guided home exercise program
Minimally Invasive / Surgical Options
- Minimally invasive cervical discectomy (selected cases)
- Posterior cervical foraminotomy (selected cases)
- Anterior cervical discectomy and fusion (ACDF)
- Cervical artificial disc replacement (selected cases)
- Decompression when clinically indicated
Recovery
Recovery depends on symptom severity and your treatment plan. Many patients improve with non-surgical care, while others may benefit from injections or surgery when nerve compression persists.
Conservative Care
- Many improve over weeks
- PT + home exercise supports long-term results
- Gradual return to activity
After Injections
- Relief may start within days to ~2 weeks
- Best paired with rehab and posture changes
- Repeat only when clinically appropriate
After Surgery
- Early mobility is encouraged in most cases
- Restrictions depend on procedure type
- PT may be recommended based on your plan
Prevention
While not every disc herniation can be prevented, consistent spine-friendly habits can reduce risk and help prevent flare-ups.
Daily Habits
- Neutral posture at desk and during phone use
- Micro-breaks from prolonged sitting
- Proper lifting mechanics
- Sleep position that avoids extreme neck angles
Strength & Mobility
- Upper back and scapular strengthening
- Deep neck flexor endurance
- Thoracic mobility work
- Low-impact conditioning consistency
Schedule a Consultation
If you have neck pain with radiating arm symptoms, numbness, tingling, or weakness, we can confirm the diagnosis and outline a plan based on your symptoms and imaging.
Request an Appointment
Request AppointmentCall the Office
Call 888-978-0985FAQ
Can a cervical disc herniation heal without surgery?
Many cases improve with time and non-surgical care focused on reducing inflammation, restoring function, and managing symptoms.
How do I know if it’s a pinched nerve?
Radiating arm pain, numbness, tingling, or weakness can suggest nerve irritation. A physical exam and MRI can help confirm the diagnosis.
What happens if therapy doesn’t help?
Next steps may include targeted injections or a surgical evaluation if symptoms persist or weakness progresses.
When should I worry?
Seek urgent evaluation for worsening weakness, balance/coordination problems, or new bowel/bladder changes.