
Lumbar Stenosis
Lumbar stenosis occurs when the spinal canal narrows in the lower back and compresses nearby nerves. It commonly causes low back pain, leg pain, numbness, and cramping with walking or standing (neurogenic claudication).
Common Symptoms
- Low back pain or stiffness
- Leg pain, numbness, or tingling
- Heaviness, cramping, or fatigue in the legs when walking
- Symptoms that improve when sitting or leaning forward
Common Causes
- Age-related degeneration and arthritis
- Bone spurs (osteophytes)
- Disc bulging or disc herniation
- Thickened ligaments and facet joint enlargement
Insurance check, handled.
We’ll verify benefits and walk you through expected coverage before treatment. No surprises.
- Benefit verification before major steps
- Clear next steps + documentation help
- Scheduling support from our team
What Is Lumbar Stenosis?
Lumbar stenosis is narrowing of the spinal canal in the lower back. This narrowing can compress the nerve roots that travel into the legs. A classic symptom pattern is pain, heaviness, or cramping in the legs with walking or standing, which often improves with sitting or leaning forward.
The most common cause is degeneration over time. Arthritis, disc changes, and ligament thickening can reduce the space available for nerves and lead to irritation or compression.
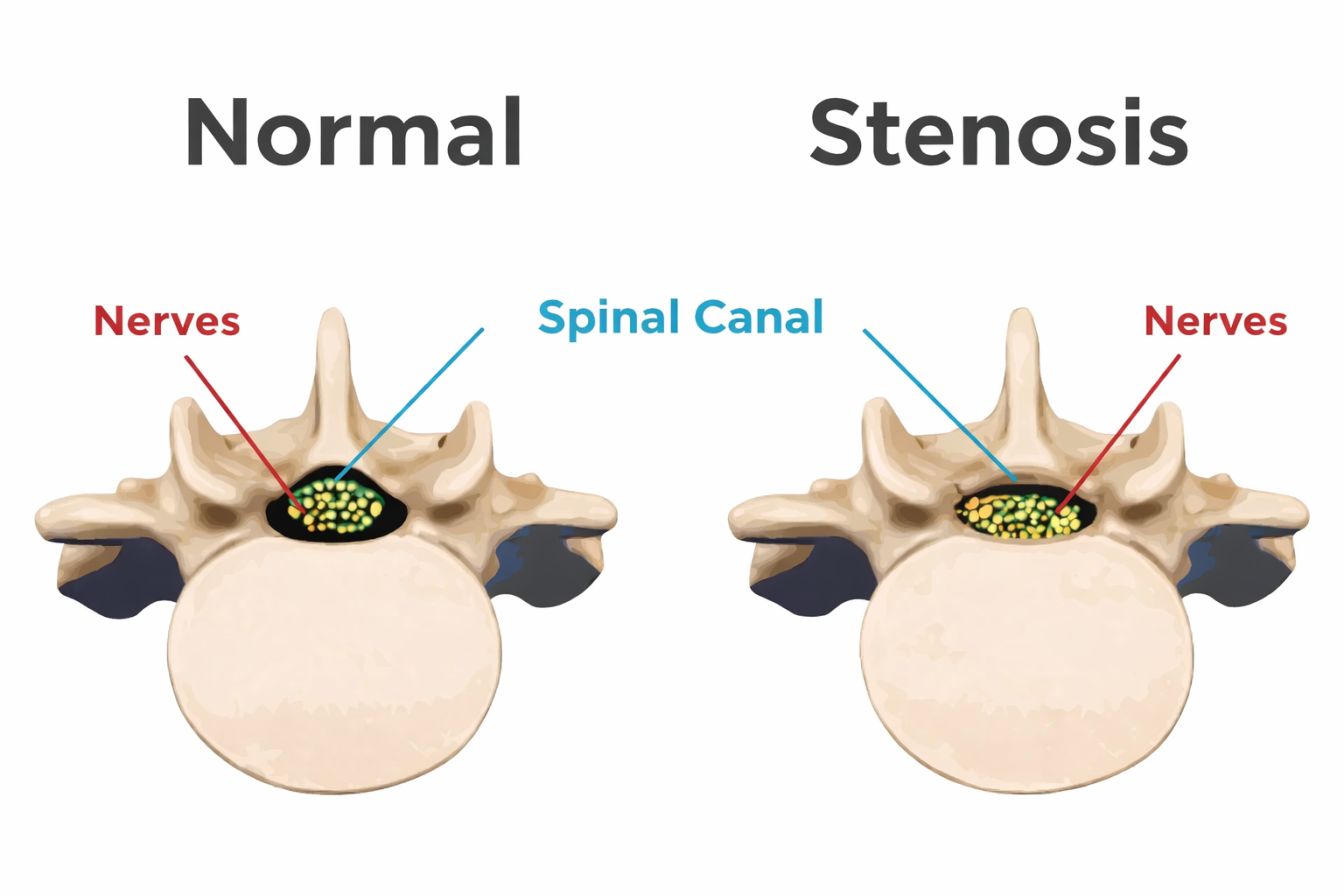
Illustration showing spinal canal narrowing (stenosis) that can compress nerves.
Why It Happens
Lumbar stenosis typically develops as discs degenerate, facet joints become arthritic, ligaments thicken, and bone spurs form. These changes can narrow the canal and compress nerve roots, especially during standing or walking.
When It Needs Prompt Evaluation
Worsening weakness, severe numbness, or new bowel/bladder changes should be evaluated promptly. These can be signs of significant nerve compression.
Symptom Check
This guided check helps sort common lumbar stenosis symptom patterns, including neurogenic claudication. It’s not a diagnosis—if symptoms are concerning, schedule an evaluation.
Lumbar Stenosis Triage
5 questions • takes about 30 seconds
1) Any urgent symptoms right now?
2) Do symptoms worsen with standing/walking?
3) Does sitting or leaning forward help?
4) Any leg pain that travels down in a line (sciatica pattern)?
5) Is weakness progressing?
Diagnosis
Diagnosis starts with a focused exam and a review of your symptoms—especially whether symptoms worsen with standing/walking and improve with sitting. Imaging confirms stenosis and helps identify the level(s) involved.
Clinical Exam
- Strength, sensation, and reflex testing
- Walking tolerance and symptom pattern review
- Assessment for nerve irritation signs
Imaging
- MRI (best for nerves and discs)
- X-rays (alignment and degeneration)
- CT or CT myelogram (selected cases)
Additional Tests
- EMG/NCS (if needed for nerve function)
- Diagnostic injections (selected cases)
Treatment
Treatment often begins with conservative care to reduce inflammation, improve mobility, and increase walking tolerance. If symptoms persist or function declines, minimally invasive or surgical decompression may be recommended.
Non-Surgical Options
- Physical therapy (core strength, mobility, conditioning)
- Activity modification and pacing strategies
- Anti-inflammatory medications (NSAIDs) when appropriate
- Short-term oral steroids (selected cases)
- Epidural steroid injections
- Selective nerve root blocks
- Heat/ice and guided home exercise program
Surgical Options
- Minimally invasive decompression (selected cases)
- Laminectomy (decompression to create more space)
- Foraminotomy (nerve root decompression)
- Decompression with stabilization/fusion when indicated
Recovery
Recovery depends on severity, duration of symptoms, and treatment choice. Many patients improve with conservative care. When surgery is needed, the goal is often to improve leg symptoms and walking tolerance.
Conservative Care
- Improvement often builds over weeks
- PT + home exercises support long-term results
- Walking tolerance can improve gradually
After Injections
- Relief may start within days to ~2 weeks
- Best paired with rehab and conditioning
- Repeat only when clinically appropriate
After Surgery
- Early mobility is encouraged in most cases
- Restrictions depend on procedure type
- PT may be recommended based on your plan
Prevention
While not every age-related change can be prevented, consistent spine-friendly habits can reduce flare-ups and support long-term lower back health.
Daily Habits
- Maintain good posture and core support
- Take breaks from prolonged sitting or standing
- Use proper lifting mechanics
- Stay active and maintain a healthy weight when appropriate
Strength & Mobility
- Core strengthening and hip mobility
- Glute and lower body strengthening
- Low-impact conditioning consistency
- Flexibility work to reduce stiffness
FAQ
What is neurogenic claudication?
Neurogenic claudication is leg pain, heaviness, cramping, or fatigue that occurs with walking or standing due to nerve compression, and often improves when sitting or leaning forward.
Does lumbar stenosis always require surgery?
No. Many patients improve with conservative care such as therapy, activity modification, and injections. Surgery is considered when symptoms persist, walking tolerance declines, or neurological deficits progress.
Why do symptoms improve when leaning forward?
Leaning forward can slightly increase space in the spinal canal and reduce nerve compression, which is why some patients feel relief when sitting or bending forward.
Are epidural steroid injections helpful for lumbar stenosis?
In selected cases, epidural steroid injections can reduce inflammation around irritated nerves and help improve walking tolerance. Results vary, and they’re typically used alongside rehab and conditioning.
Schedule a consultation
We’ll review your symptoms, imaging, and options. If walking tolerance is dropping or weakness is worsening, mention that when scheduling.
If you have new bowel/bladder changes or rapidly worsening weakness, seek urgent evaluation.
What to bring
- Prior MRI/CT reports (if available)
- Medication list
- Walking tolerance details (how far before symptoms?)
- Any weakness/numbness notes (what’s changing?)