
Degenerative Disc Disease (DDD)
Degenerative disc disease (DDD) is wear-and-tear of the spinal discs. As discs lose hydration and height over time, they can trigger inflammation, stiffness, and pain—and in some cases irritate nearby nerves causing arm or leg symptoms.
Common Symptoms
- Neck or low back pain that comes and goes
- Stiffness (often worse in the morning or after sitting)
- Pain with bending, lifting, prolonged sitting
- Sometimes: radiating arm/leg pain, numbness, tingling
Common Causes
- Disc dehydration and loss of height over time
- Annular tears (small disc wall tears)
- Disc bulge/herniation (selected cases)
- Genetics, smoking, repetitive strain (risk factors)
Insurance check, handled.
We can verify benefits, help coordinate imaging, and explain next steps once results are in.
- Benefit verification before procedures
- Help coordinating MRI orders
- Clear plan after imaging
What Is Degenerative Disc Disease?
Discs are shock absorbers between vertebrae. With time, discs can lose water content and height, becoming less flexible. That change can increase load on surrounding joints and create inflammation that feels like deep, aching neck or back pain.
DDD is common on imaging and doesn’t always cause symptoms. When symptoms occur, they may come from disc inflammation, abnormal motion at a spinal segment, or narrowing that irritates nearby nerves.
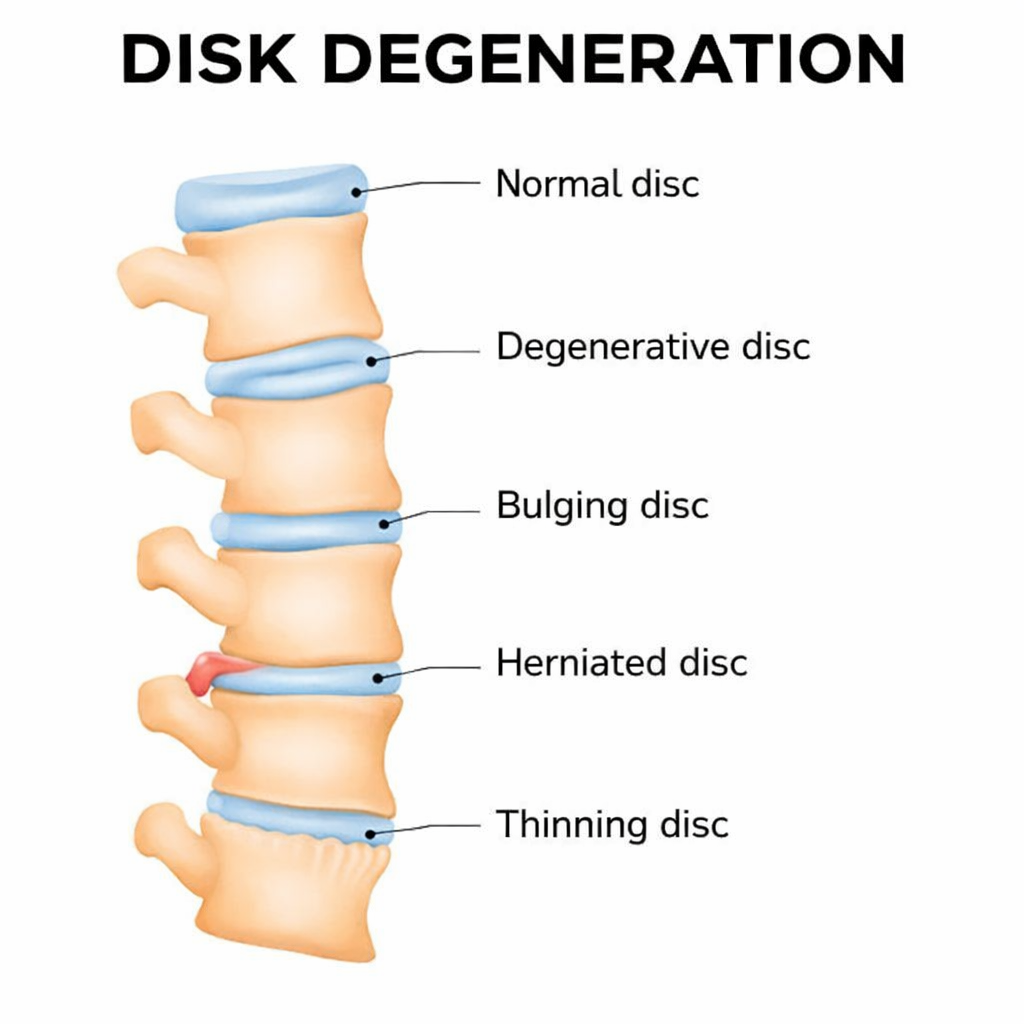
Illustration showing disc degeneration and reduced disc height.
Why It Hurts
Degenerated discs can become inflamed and pain-sensitive. Loss of disc height can also increase stress on facet joints. If narrowing develops, nerves may be irritated, causing radiating symptoms into the arms or legs.
When It Needs Prompt Evaluation
New or worsening weakness, severe numbness, trouble walking, or bowel/bladder changes should be evaluated promptly.
Quick Check
This is a quick screening to help decide urgency. Not a diagnosis.
DDD Symptom Check
5 questions • flags urgent vs routine evaluation
1) Any bowel/bladder changes or saddle numbness?
2) Any weakness or rapidly worsening numbness?
3) Any fever/chills, unexplained weight loss, or history of cancer?
4) Is pain severe and not improving with rest/meds?
5) How long have symptoms been going on?
Diagnosis
Diagnosis starts with a physical exam and symptom review, then imaging to confirm degeneration and determine whether nerves are involved. The goal is to identify the pain generator and rule out more serious causes.
Clinical Exam
- Pain pattern and functional limitations
- Range of motion and mechanical triggers
- Strength, sensation, reflex testing (when indicated)
Imaging
- X-rays (disc height, alignment, instability clues)
- MRI (discs, nerves, stenosis, inflammation)
- CT (selected cases)
Helpful Add-ons
- Diagnostic injections (selected cases)
- EMG/NCS if symptoms are unclear
- Review of prior imaging if available
Treatment
Most patients improve without surgery. Treatment focuses on reducing inflammation, restoring mobility, and building durable core/hip strength so the spine tolerates daily activity better.
Non-Surgical Options
- Physical therapy (core stability, mobility, conditioning)
- Ergonomic and activity modifications
- Anti-inflammatory medications (NSAIDs) when appropriate
- Guided home exercise program
- Injections for pain control (selected cases)
Surgical Options (Selected Cases)
- Considered when pain persists despite structured care or neurologic compression is present
- Options may include decompression and/or fusion depending on findings
- Approach is tailored to the level and severity
Recovery
Improvement is usually gradual. Consistency with rehab is the biggest driver of long-term success.
Conservative Care
- Flares can happen — plan around them
- Walking and light activity often helps
- Strength gains build over months
After Injections
- Relief may start within days to ~2 weeks
- Best paired with strengthening
- Repeat only when clinically appropriate
When to Recheck
- New radiating pain or weakness
- Worsening walking tolerance
- No improvement despite structured plan
Prevention
You can’t stop aging, but you can reduce flare-ups by improving mechanics and strengthening the system around the spine.
Daily Habits
- Break up prolonged sitting
- Use proper lifting mechanics
- Optimize workstation ergonomics
- Quit smoking (if applicable)
Strength & Mobility
- Core + hip strengthening
- Mobility work for stiffness
- Low-impact conditioning consistency
- Progress gradually
FAQ
Is DDD “normal” on imaging?
Disc degeneration is common with age. Many people have it on MRI without pain. Symptoms depend on the person and the mechanics of the spine.
Does DDD always get worse?
Imaging changes can progress, but symptoms don’t always. Many patients do well long-term with conditioning and strength work.
When is MRI needed?
MRI is most helpful when there are radiating symptoms, neurologic findings, or persistent pain that isn’t improving with conservative care.
Schedule a consultation
We’ll review symptoms and imaging and coordinate the safest next step.
If you have weakness, saddle numbness, or bowel/bladder changes, seek urgent evaluation.
What to bring
- MRI/X-ray reports and image links/discs (if available)
- Medication list
- Timeline of symptoms and prior treatments
- Any prior operative records (if applicable)